Evaluation
Three cluster-randomized controlled trials (RCTs) will be conducted to determine the effectiveness of an integrated nutrition-sensitive and nutrition-specific program on health and environmental outcomes. We will include four public secondary schools in each of the three cities in SSA, namely Ouagadougou (Burkina Faso), Dar es Salaam (Tanzania), and Kisumu (Kenya). At each study site, two schools will receive the intervention program and two schools will serve as the control group and thus, will receive the ‘standard of care’, which refers to the mass media campaign only. We will implement the intervention over a period of one academic year, after careful co- design (WP2, WP3, WP4). We will screen secondary schools in the catchment area of the existing Health and Demographic Surveillance Systems (HDSS) in the three cities for their eligibility. Eligibility criteria are: being a public school, no existing urban farming, availability of water and land to establish a garden all year round, and no existing/implemented curriculum on nutrition and environmental protection. We will select and match schools according to their similarities in size (number of students) and geographic location (formal or informal settlement). In close collaboration with WP4 and WP6, we will approach the headmasters/mistress, parents, and other stakeholders of the schools for sensitization (purposes, procedures, risks and benefits, voluntariness). We aim to enroll 190 adolescents (11-16 years) per school, amounting to a total sample size of 760 students.
We will conduct baseline and endline surveys among all students and one of their parents, respectively. Trained data collectors will use standardized questionnaires and interview guides, which will be translated into the national official languages and additional local languages, if needed. Electronic data collection will be supported by digital software. In each of the four schools per country, we will enroll 190 students between the ages of 11-16 years old. As an innovation in Changemaker, we will determine the effects on undernutrition and overnutrition employing a validated, non-invasive assessment tool that captures both ends of the anthropometric continuum: The mid-upper arm circumference (MUAC) z-score tape.
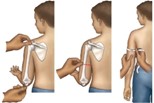 A: MUAC measurement by trained personnel
A: MUAC measurement by trained personnel
 B: Using the MUAC z-score tape.
B: Using the MUAC z-score tape.
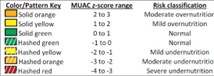 C: Color coding and risk classification of the MUAC z-score tape.
C: Color coding and risk classification of the MUAC z-score tape.
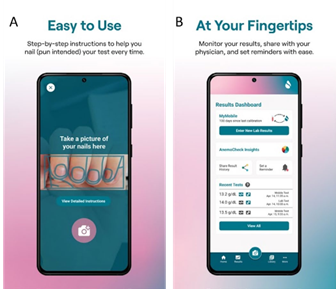
In addition, we will employ a technological innovation for non-invasive self-assessment of hemoglobin concentration (Hb); the Sanguina Smartphone
Application. The application estimates Hb concentration via color-sensitive, algorithm-based analysis of fingernail bed images. Hb is an important lifestyle marker that reflects dietary intake, exposure to infectious diseases, and healthcare uptake.
For the assessments of dietary behavior and physical activity, we will employ approaches that balance feasibility and validity. Dietary intake will be determined by a 134-items Food Propensity Questionnaire (FPQ) that is validated for a multi-ethnic population in Europe and was adapted to the contexts in Dar es Salam, Ouagdougou, and Kisumu. Changemaker will apply a simple pedometer App as a monitor-based assessment tool. They are objective and quantify the steps performed as an indicator of movement. Pedometers track vertical hip movements that are recorded as steps and the data usually can be stored for 24 hours or several days depending on the pedometer.
Public health innovations that are evidence-based may not achieve the desired results when they are poorly implemented. For measuring implementation success, it is therefore necessary to distinguish between innovation and implementation effectiveness. Implementation effectiveness can be defined as consistency and quality in how targeted organization members use a particular innovation. Implementation outcomes can be measured by examining acceptability, adoption, appropriateness, feasibility, fidelity, penetration, and sustainability. During our integral process evaluation, we will identify what happened during the implementation process that might have affected not just the impact of the intervention, but also other implementation science outcomes. These indicators will include:
- The acceptability of the intervention content by the school community,
- The feasibility of delivering the intervention activities in schools and communities,
- Fidelity of intervention delivery,
- Uptake of intervention activities by the school system,
- Coverage of and participation in intervention activities by the school community,
- Perceived relevance and usefulness of the intervention activities by the school community, and
- Maintenance of and willingness to continue the intervention activities in schools and beyond.
Along with these indicators, we will also identify the causal mechanisms that produce change and the factors that enable the intervention implementation.
The implementation evaluation will be theoretically guided by the Practical, Robust Implementation and Sustainability Model framework for implementation of Changemaker (PRISM) framework as described below:
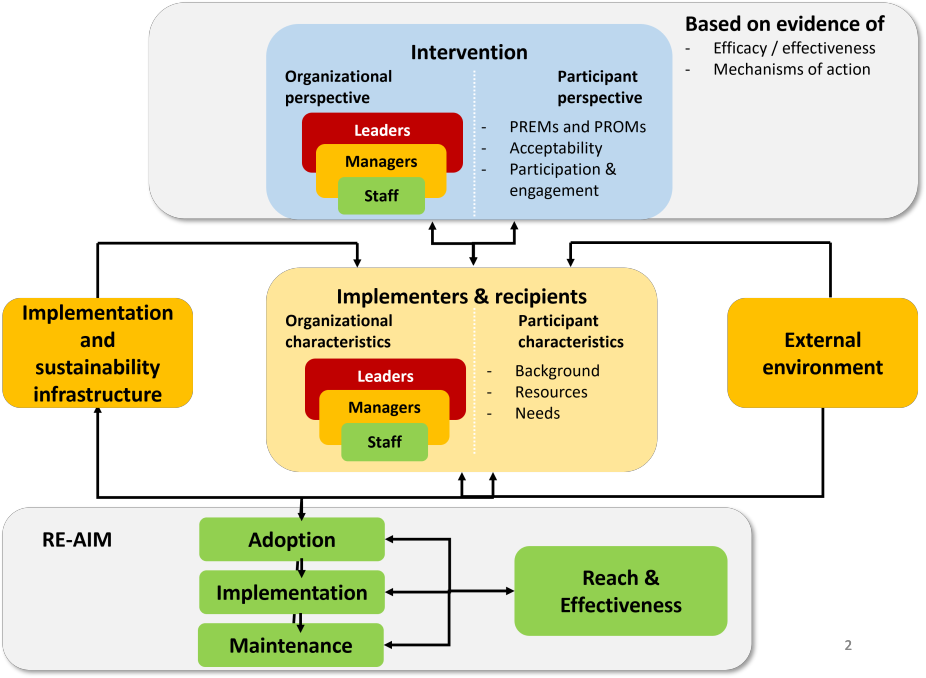
By utilizing the PRISM framework, we will develop a Theory of Change model to evaluate how the Changemaker intervention interacts with the primary beneficiaries (i.e., students), the school community (i.e., school leaders, teachers, parents, and other community members) and the system (physical environment, and procedures and policies) to influence program adoption, implementation, maintenance, reach, and effectiveness.
We will cost the implementation of Changemaker by calculating the direct and indirect costs (productivity loss) from a societal perspective as appropriate. The WHO-CHOICE methodology, a standard for conducting economic analysis for health-related programs, will be followed to assess implementation costs. A mixed methodology will be applied to measure the different cost components. A micro simulation model will be adapted to predict the future health outcomes (in terms of obesity progression) and associated costs on an individual level. The data predicting individual BMI change for the model will come from a literature review. Adulthood overweight prevention will lead to health-related quality of life (HRQoL) improvement, which will be estimated and accounted for in a cost-utility analysis. Epidemiological and cost data will be used to inform the model and predict the cost-effectiveness of Changemaker. Incremental cost-effectiveness ratio (ICER) will be calculated (the ratio of incremental intervention costs divided by the total number of QALYs saved).
Updated by:
Webmaster 2024-10-30